

For those who dedicate themselves to a job that involves frequent moves between one country and another, for example the expats who go on humanitarian or military missions, to the factors listed above is added the whole process, often unexpected and therefore of great impact, of the re-adaptation upon the return.
After work experience in another culture, you can feel a series of sometimes-conflicting feelings. In fact, the joy of returning and the desire to rest may be accompanied by other less pleasant feelings. It is usual to feel confused, disoriented, lost, upset, frustrated with regard to the materialism of Western countries. You may have the feeling that the expectations you had before you left were not fulfilled, or even you may have had to return earlier than expected.
You may feel depressed and constantly remember the experiences you had in the field, or what you lived on a mission may seem unreal and far away.
It is often very difficult to try to communicate the experience you lived to those around you. It may happen, for example, that when you start telling your friends and relatives about your experience, you have a feeling of lack of interest from them side.
Another important change that you may feel is to go back to being “one of many” and find yourself more alone. In the field, you most probably lived 24/7 with other people, while the return to your usual place of residence can mean not always having someone next to you, having to find a specific moment during the week to meet with friends or do activities with other people, and this can make you feel alone.
All this requires a process of re-adaptation to your environment that may cause feelings of sadness and loss.
When you are far from the place where you habitually reside and you consider as one of your homes, you preserve a frozen mental image of what your life is like there and, when you return, you face the fact that there have been changes. It may happen that the appearance of the city has changed, or that the life situation of the people you know did. Recovering the social network is a double process of adaptation, by your side and by the one of those who have remained “at home”.
Upon the return it is important that you take care of yourself, of your health on all levels, it is in this moment where you are most exposed and vulnerable.
A psychological accompaniment is indicated when you feel at risk of distress, in order not to arrive at a state of excessive accumulation of distress, which would result in a burnout, with consequent malaise in the whole of life.
If you already feel in a state of burnout, compassion fatigue / vicarious trauma, the psychotherapeutic path will help you to regain confidence in yourself, to feel again capable of love and to grasp the beauty of what surrounds you.
Burnout, compassion fatigue/vicarious trauma, Acute Stress Disorder (ASD), Post-Traumatic Stress Disorder (PTSD), complex PTSD
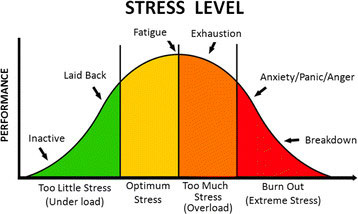
Burnout is a state resulting from a multifactorial process of a long-lasting exposure, in a professional setting, to continuous stress. It is mainly due to an imbalance between the demands and the means the person has to satisfy them, in other words, to a lack of reciprocity between the expectations and the real possibilities. The state of burnout has three main components:
Exhaustion: a state of being extremely tired
Cynicism: indifference and detachment towards others (beneficiaries and/or colleagues)
Inefficacy: feeling like one is not accomplishing anything worthwhile at work that may can lead to a lack of motivation
Burnout is a state; however, it raises from a long process consisting of 3 stages: